Overview - Best Heart Surgery Hospital in Bangalore
Sparsh is recognised as the best heart surgery hospital in Bangalore, offering advanced and patient-focused care for a wide range of cardiac conditions. With a strong team of experienced cardiac surgeons, cardiologists, and critical care specialists, we provide comprehensive heart surgery in Bangalore supported by modern infrastructure and evidence-based protocols.
As Bangalore’s best hospital for cardiac surgery, Sparsh focuses on precise diagnosis, personalised treatment planning, and improved recovery outcomes. From routine procedures to complex cardiac surgeries, our multidisciplinary approach ensures safe and effective care. Patients benefit from advanced surgical techniques, dedicated cardiac ICUs, and continuous monitoring, making Sparsh a trusted choice for high-quality cardiac treatment.
Types of Cardiac Surgery We Perform
At Sparsh, we offer a wide range of cardiac procedures designed to treat both common and complex heart conditions. Our expertise includes bypass surgery in Bangalore, commonly performed as CABG, to restore blood flow in blocked arteries.
We also perform heart valve surgery in Bangalore for conditions such as valve stenosis and regurgitation, along with congenital heart surgery for structural defects present from birth. Advanced procedures like aortic surgery help manage aneurysms and other aortic conditions, while arrhythmia surgeries address abnormal heart rhythms.
Additionally, we specialise in beating-heart surgery in Bangalore, which allows certain procedures to be performed without stopping the heart, thereby reducing recovery time. Each treatment is planned based on the patient’s condition to ensure safe outcomes and long-term heart health.
Minimally Invasive & Advanced Heart Surgery
Sparsh offers minimally invasive cardiac surgery in Bangalore using advanced surgical techniques that reduce the need for large incisions. These procedures are designed to minimise pain, shorten hospital stays, and support faster recovery.
Our team also performs beating-heart surgery in Bangalore, where procedures are performed without stopping the heart, improving safety for selected patients. Using high-precision instruments and modern operating systems, we ensure accurate surgical outcomes. This innovative approach allows patients to return to daily activities sooner while maintaining high standards of care and clinical effectiveness.
Emergency Cardiac Surgery & Critical Care
Sparsh provides the best emergency cardiac surgery in Bangalore with round-the-clock readiness for critical heart conditions. Our cardiac emergency team is equipped to handle heart attacks, acute coronary events, and life-threatening complications with immediate intervention.
As a leading heart surgery hospital in Bangalore, we offer advanced cardiac ICUs, continuous monitoring, and rapid surgical support. Technologies like ECMO are used when required to support heart and lung function in critical situations. Our integrated approach ensures timely treatment, stabilisation, and improved survival outcomes for patients with cardiac emergencies.
ECMO & Mechanical Circulatory Support
As an advanced cardiac surgery hospital, Sparsh offers ECMO (Extracorporeal Membrane Oxygenation) and mechanical circulatory support for critically ill patients. These technologies temporarily support heart and lung function when conventional treatments are not sufficient.
ECMO is used in complex cardiac emergencies, post-surgical recovery, and severe heart failure cases. Our specialised team ensures careful monitoring and management throughout the treatment process. This advanced support system enhances survival chances and provides a bridge to recovery or further treatment when needed.
Conditions Treated with Cardiac Surgery
At Sparsh, a trusted cardiac surgery hospital in Bangalore, we treat a wide range of heart conditions requiring surgical intervention. These include coronary artery disease, heart valve disorders, congenital heart defects, heart failure, and aortic aneurysms.
Our approach to heart surgery in Bangalore focuses on early diagnosis, accurate evaluation, and timely intervention. Each patient receives a personalised treatment plan based on their condition and overall health. With advanced surgical expertise and comprehensive care, we aim to improve long-term heart function and quality of life.
Why Choose SPARSH Hospital for Heart Surgery?
Sparsh is regarded as one of the best cardiac surgery hospitals in Bangalore, known for its experienced team, advanced technology, and patient-focused care. Our cardiac surgeons, cardiologists, and critical care specialists work together to deliver precise and effective treatment.
As a top heart surgery hospital in Bangalore, we offer modern operating theatres, advanced imaging, and dedicated cardiac ICUs to support complex procedures. Our focus on safety, clinical excellence, and personalised care ensures better outcomes and faster recovery. Patients trust Sparsh for its transparent approach, evidence-based treatments, and commitment to delivering high-quality cardiac care.
Cost of Heart Surgery in Bangalore
The cost of open heart surgery in Bangalore and the CABG surgery cost in Bangalore can vary depending on several factors. These include the type of procedure, the patient’s medical condition, hospital infrastructure, the surgeon’s expertise, and the duration of hospital stay.
At Sparsh, we focus on providing transparent cost estimates and personalised treatment plans. Additional factors such as pre-surgical tests, post-operative care, and ICU support may also influence the overall cost. Our goal is to ensure patients receive high-quality cardiac care with clarity and financial guidance throughout their treatment journey.
Cardiac Surgery Hospital Near You
Looking for an open heart surgery hospital near me? Sparsh offers advanced cardiac surgery services across multiple locations, ensuring expert care close to you.
We provide cardiac surgery in Infantry Road, Hennur, RR Nagar, Yelahanka, and Yeswanthpur. Each centre is equipped with experienced specialists, modern operating theatres, and comprehensive cardiac care facilities.
With easy accessibility and consistent quality across locations, Sparsh ensures that patients receive timely diagnosis, expert surgical care, and seamless recovery support near their home.
An Innovative Approach to Treatment

Complex Heart Surgery with International Quality of Care

Minimally Invasive Heart Surgery
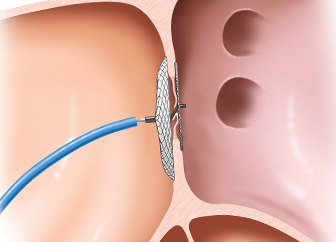
Device Closure of Congenital Defects

Complex Coronary Interventions
Hybrid Procedures with Cardiologists and Surgeons
We Specialise in the Treatment of
- Cardiac Evaluation
- Cardiac Wellness Assessment
- Coronary Interventions
- CABG
- Valve Repair/Replacement Surgery
- Arrhythmia Treatment
- Aortic Aneurysm Surgery
- Device Closure of ASD, VSD, PDA
- Balloon Dilatation of Coarctation
- Valve Stenosis
- RVOT With or Without Stenting
- Congenital Heart Disease Diagnosis
- Resuscitation and Treatment
- Truncus Arteriosus Surgery