Overview
Sleep dentistry is an emerging interdisciplinary domain that plays a crucial role in the identification and management of sleep-related breathing disorders, particularly Obstructive Sleep Apnea (OSA). OSA is characterized by recurrent upper airway obstruction during sleep, leading to significant systemic morbidity. Dentists, especially orthodontists and maxillofacial surgeons, are uniquely positioned to identify craniofacial and intraoral risk factors contributing to airway compromise. This article provides a comprehensive overview of airway assessment, including craniofacial morphology, soft tissue evaluation, bruxism, and the impact of maxillary constriction on breathing. It further discusses diagnostic protocols and outlines both non-surgical and surgical mandibular advancement strategies, including oral appliance therapy, growth modification, MARPE, SARPE, and maxillomandibular advancement. Emphasis is placed on the role of dentists in early detection and multidisciplinary management of OSA.
Introduction
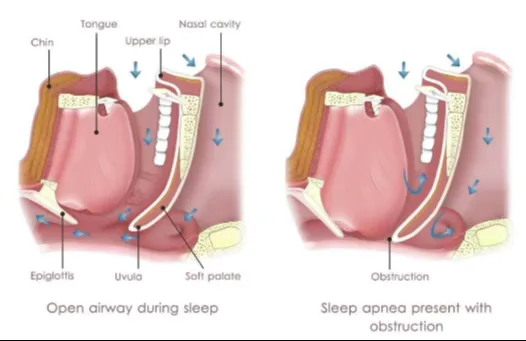
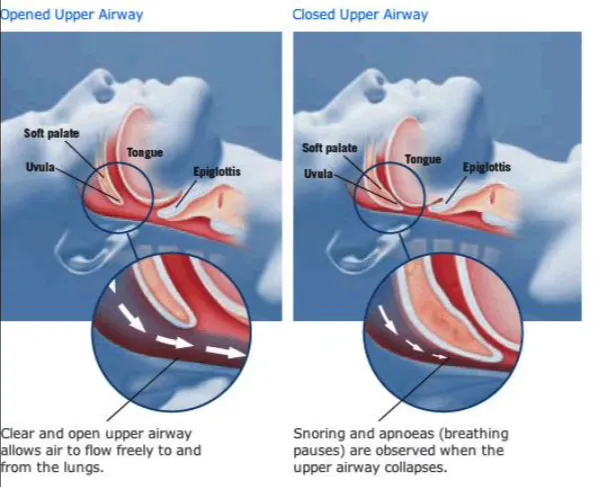
Sleep-related breathing disorders (SRBDs) encompass a spectrum of conditions that impair normal respiration during sleep, with Obstructive Sleep Apnea (OSA) being the most prevalent. OSA is defined by repetitive episodes of partial or complete upper airway obstruction, resulting in intermittent hypoxia, sleep fragmentation, and increased sympathetic activity. The condition is associated with significant systemic complications, including cardiovascular disease, hypertension, stroke, and metabolic disorders.
Dentists are often the first healthcare professionals to identify anatomical and functional indicators of airway compromise. Sleep dentistry integrates dental expertise with sleep medicine to facilitate early diagnosis and management, particularly through airway-focused orthodontic and surgical interventions.
Patients with OSA commonly present with:
- Loud snoring
- Witnessed apneas
- Excessive daytime sleepiness
- Morning headaches
- Xerostomia
- Cognitive impairment
From a dental perspective, additional findings include:
- Bruxism
- Scalloped tongue
- Narrow maxillary arch
- Retrognathic mandible
Airway Assessment in Dental Practice
Craniofacial Morphology
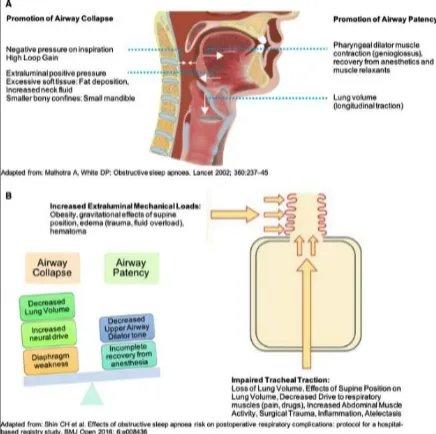
Craniofacial skeletal relationships significantly influence airway patency. High-risk features include:
- Retrognathic mandible causing posterior tongue displacement
- Maxillary constriction reducing nasal airway volume
- Vertical growth pattern increasing airway collapsibility
- High-arched palate decreasing nasal cavity width
Assessment includes clinical profile analysis, cephalometric measurements (SNA, SNB, ANB, posterior airway space), and three-dimensional imaging such as CBCT when indicated.
Soft Tissue Evaluation
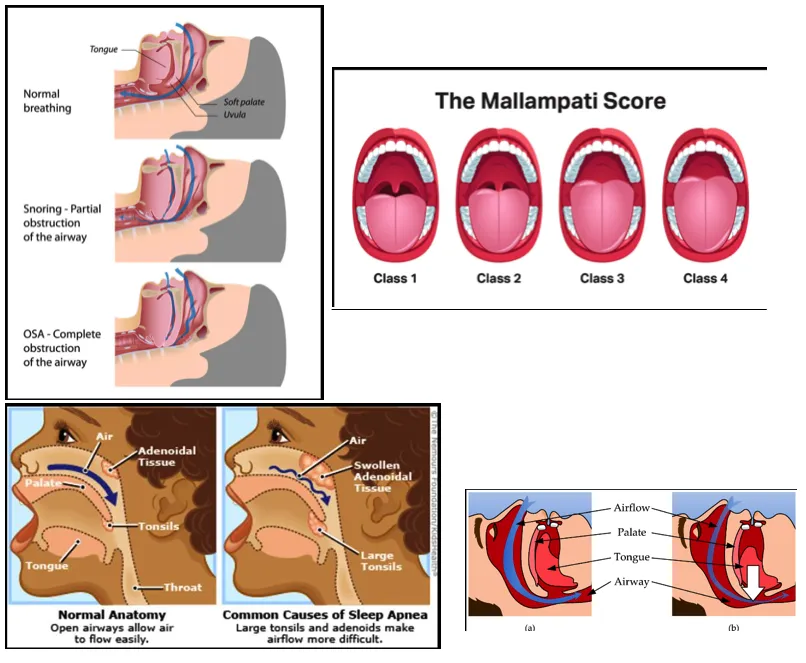
Soft tissue structures are often the primary contributors to airway obstruction. Key components include:
- Tongue size and posture (macroglossia, posterior positioning)
- Soft palate length and thickness
- Tonsillar hypertrophy, especially in children
- Adipose tissue deposition in the pharyngeal region
Clinical tools such as the Mallampati classification, Friedman tongue position, and tonsillar grading are routinely employed.
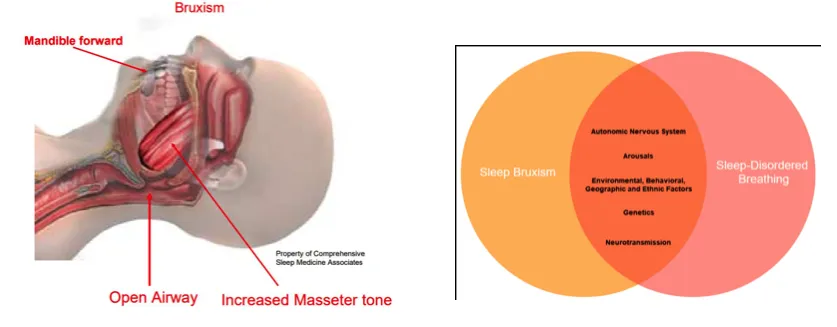
Bruxism and Airway Dynamics
Sleep bruxism is increasingly recognized as a physiological response to airway obstruction. Episodes of airway collapse trigger micro-arousals, leading to mandibular advancement and activation of masticatory muscles to restore airway patency. Clinically, this presents as occlusal wear facets, masseter hypertrophy, tongue scalloping, and morning jaw discomfort.
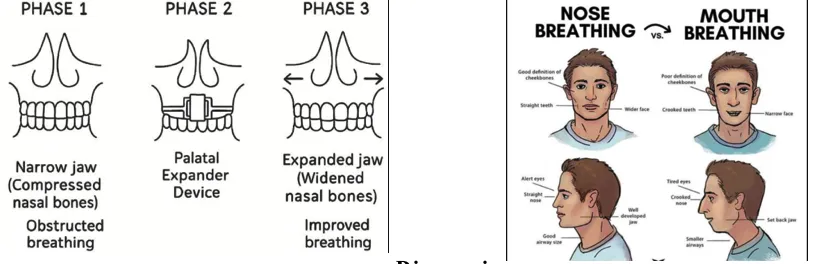
Maxillary Constriction and Pediatric Airway
A narrow maxillary arch reduces nasal cavity width and increases airway resistance, promoting mouth breathing. In children, this results in a cascade of functional and structural changes, including altered tongue posture, impaired craniofacial development, and increased risk of sleep-disordered breathing. Orthodontic interventions such as rapid maxillary expansion (RME/MARPE) have been shown to improve nasal airflow and airway dimensions
Diagnosis of OSA
Initial screening involves validated questionnaires and definitive diagnosis is established through polysomnography (PSG), the gold standard, or home sleep apnea testing (HSAT).
Severity is determined using the Apnea-Hypopnea Index (AHI):
- Mild: 5–15 events/hour
- Moderate: 15–30 events/hour
- Severe: >30 events/hour
Management Strategies in Sleep Dentistry
Management of OSA requires a multidisciplinary approach, with dentists playing a central role in non-invasive and adjunctive therapies.
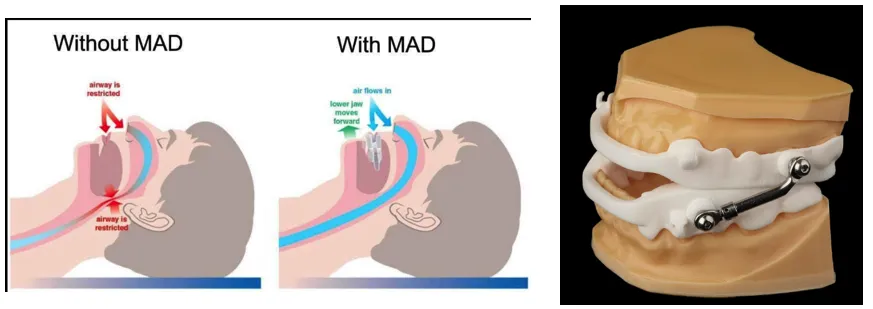
Oral Appliance Therapy
Mandibular advancement devices (MADs) are custom intraoral appliances that reposition the mandible anteriorly during sleep. This forward positioning increases airway dimensions, reduces collapsibility, and improves oxygen saturation. MADs are indicated in patients with mild to moderate OSA and those intolerant to continuous positive airway pressure (CPAP) therapy
Orthodontic Interventions
Growth Modification
In pediatric patients, functional appliances such as Twin Block and Herbst appliances promote mandibular growth, improving sagittal jaw relationships and airway dimensions.
Maxillary Expansion
Miniscrew-assisted rapid palatal expansion (MARPE) facilitates skeletal expansion of the maxilla, enhancing nasal airflow and reducing airway resistance, particularly in adolescents and young adults.
Surgical Interventions
SARPE (Surgically Assisted Rapid Palatal Expansion)
Indicated in skeletally mature patients, SARPE increases maxillary width and nasal airway volume.
Mandibular Advancement Surgery (BSSO)
Bilateral sagittal split osteotomy allows permanent advancement of the mandible, significantly increasing posterior airway space.
Maxillomandibular Advancement (MMA)
MMA is considered the gold standard for moderate to severe OSA. By advancing both jaws, it enlarges the entire upper airway and significantly reduces airway collapsibility, with reported success rates exceeding 85–90%.
Adjunctive Procedures
Procedures such as genioglossus advancement and hyoid suspension further stabilize the airway and are often performed in conjunction with MMA
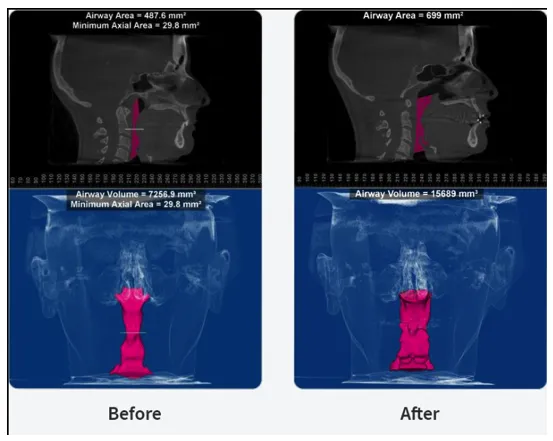
Biological Basis of Mandibular Advancement
Mandibular advancement exerts its therapeutic effect through anatomical and functional changes:
- Forward displacement of the tongue via the genioglossus muscle
- Stabilization of the hyoid bone
- Increased tension in the pharyngeal walls
- Enlargement of the velopharyngeal and oropharyngeal airway
These changes collectively reduce airway obstruction during sleep.
Role of the Orthodontist and Maxillofacial Surgeon
Orthodontists are instrumental in early detection, growth modification, and airway-focused treatment planning. Maxillofacial surgeons provide definitive correction in severe cases through skeletal advancement procedures. Collaboration between dental and medical professionals is essential for optimal outcomes.
Clinical Significance and Early Intervention
Untreated OSA has profound systemic implications, including cardiovascular morbidity, metabolic dysfunction, and reduced quality of life. Early identification and intervention by dental professionals can alter disease progression, particularly in pediatric populations, and reduce the need for invasive treatments in adulthood.
Conclusion
Sleep dentistry represents a paradigm shift toward airway-centered diagnosis and management. Comprehensive airway assessment, combined with orthodontic and surgical mandibular advancement strategies, provides effective solutions for patients with OSA. Dentists play a pivotal role in the multidisciplinary management of this condition, contributing significantly to improved patient outcomes and overall health.